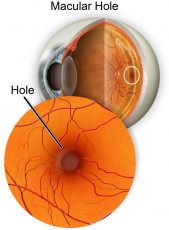
As we age, the vitreous gel can shrink and pull towards the centre of your eyeball. In some people, the vitreous gel is firmly attached to the macula and this pull can lead to the structurally weak macula to open up into a partial hole (lamellar hole) or full thickness hole.
This hole may result in a central blind spot or waviness in vision. If left untreated, a macular hole can enlarge over time causing increasing central blindness, while peripheral vision remains normal.
Macular Holes require surgery to fix, and often requires a period of posturing with gas to ensure full closure of the hole – read more about vitrectomy surgery and macular holes.
Think of the retina like a ‘wallpaper’ attached to inner shell of the eye.
A retinal tear occurs when a break in the ‘wallpaper’ forms. If the ‘wallpaper’ is still attached on the wall of the eye, the tear can be sealed off with a laser procedure, mitigating the need for an operation.
A retinal detachment occurs when intraocular fluid has gone under a retinal tear, ripping the ‘wallpaper’ off the wall. A retinal detachment is an ocular emergency that can cause permanent vision loss. You must seek urgent medical attention.
The aim of retinal detachment surgery is to halt the progression of vision loss by reattaching the retina to the back of the eye –read more about retinal tears and detachments.

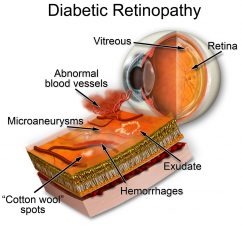
Diabetic retinopathy is a serious and sight-threatening disease that affects the blood vessels inside the retina. It is the most common form of blindness in Australians under the age of 50, with duration of diabetes and less-optimal control of diabetes major risk factors.
Diabetic retinopathy occurs as a result of oxidation damage to blood vessels due to high blood glucose. This results in a reduced ability to deliver oxygen and nutrients to retinal tissue and can lead to formation of malformed blood vessels which often leak blood into the retina.
These factors can lead to permanent injury to the highly metabolic tissue of the retina and can even result in sequelae such as retinal detachment, cataracts, and macular oedema, all of which can cause a reduction in vision.
Mild to moderate grades of diabetic retinopathy are managed with close observation and optimizing control of blood glucose levels, whilst severe or proliferative grades can require retinal laser or intravitreal injections – read more about the three main types of diabetic retinopathy.
Macular degeneration, commonly referred to as age-related macular degeneration (ARMD), affects the central vision.
It occurs as a result of accumulation of waste products and oxidation damage to the supporting tissue layer of the retina, the retinal pigmented epithelium (RPE). As this layer becomes damaged, the photoreceptors will also become irreversibly damaged.
There are two main types of age-related macular degeneration (ARMD):
– Dry ARMD is a gradual and progressive degeneration of the light-sensitive photoreceptors located at the macula, slowly reducing vision.
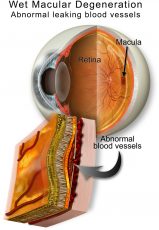
– Wet (neovascular) ARMD is the development of abnormal and highly fragile blood vessels under the retina that leak or bleed resulting in a rapid reduction and distortion of vision.
Treatment is required urgently and usually consists of intravitreal injections with medications designed to stabilise these leaky blood vessels.
While anyone can develop age-related macular degeneration, several factors can place you at greater risk – read more about macular degeneration risk factors and treatment options.
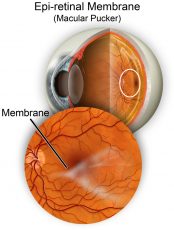
An Epiretinal Membrane, or macular pucker, is thin layer of tissue that has formed over the macula. Over time these cells contract, pull and crinkle the macula, which result in blurry and ‘wavy’ central vision.
In many cases, the symptoms of vision distortion and blurriness are mild, so no treatment is necessary although regular monitoring, especially with a Amsler grid chart, is advised.
Vitrectomy surgery may be recommended if an epiretinal membrane progresses quickly or cause significant vision deterioration – read more about epiretinal membrane symptoms and causes.
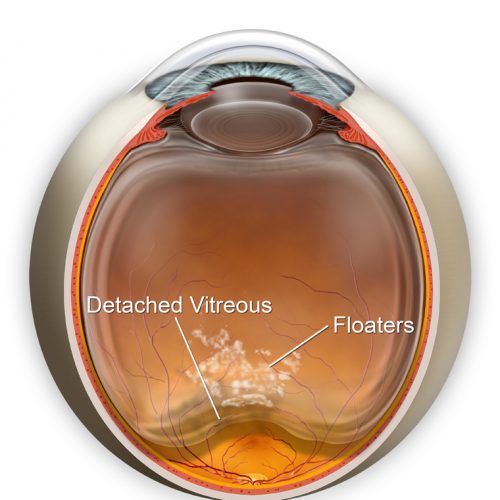
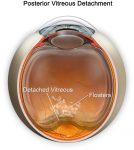
A Posterior Vitreous Detachment or PVD is a natural and common occurrence with age and happens when the vitreous gel begins to shrink and eventually separates from the retina.
The most common symptom of PVD is blurred vision from a sudden increase or change in floaters which often appear as dark dots, specks, cobwebs, or squiggly lines that move across your field of vision. You may also notice flashes like lightning or a camera flash in your peripheral vision.
Unlike a migraine, this occurs in one eye at a time.
These symptoms will usually settle down over about two months. Though the perception of floaters will improve over this time, they will never completely disappear. Most people are not too bothered, but some are, depending on where the floater settles relative to the visual axis. If bothersome, the floaters can be eradicated – speak to your vitreoretinal surgeon about this.
However, as symptoms of a PVD can mimic those of a more serious sight-threatening conditions such as retinal detachment, you should schedule an eye exam with your Optometrist or Ophthalmologist for a full examination with pupil dilation within 3-4 days to ensure no other issues are present – read more about the causes and treatment options for a posterior vitreous detachment.
Read more about other retinal conditions, including, Retinal Vein Occlusion, Retinal Artery Occlusion, and Central Serous Retinopathy.